Engineers are available to assist.

Case Studies / A Low-Cost, Handheld Retinal Camera for Screening Premature Infants in Low-Resource Settings
By Teo Kakabadze, Samer Marmash, Clin Vadakkal Shaiju & Alisha Sankhe
Team Retinex, Rice University | [email protected]
The future depends on scalable screening.
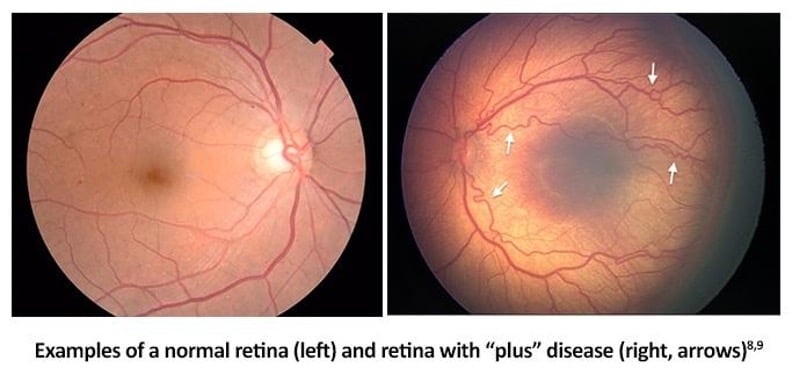
About 15 million babies are born prematurely every year. As neonatal care has improved around the world, more babies are surviving, particularly in regions where such babies previously had limited chances. As a result, Retinopathy of Prematurity (ROP), a disease once rare outside high-income countries, has now become a leading cause of childhood blindness globally. ROP is caused by abnormal blood vessel growth in a premature infant's retina. In severe cases, those vessels can pull on the retina and detach it, causing permanent blindness. The condition is treatable with laser therapy, but only if it's caught in time, typically within a few weeks of the critical developmental window. After that, the damage is irreversible.
In Kenya, a hospital-based study found that 41.7% of screened premature infants had ROP1 – a prevalence comparable to high-income countries, occurring in a setting where the infrastructure to screen for it barely exists. Researchers studying sub-Saharan Africa have warned of a full-scale ROP epidemic this decade.2 The problem isn't awareness. It's access. The development of our handheld retinal camera “Retinex” aims to shift retinal screening from specialist-only tertiary hospitals to bedside neonatal care environments, enabling earlier intervention in regions where ophthalmologists and retinal imaging systems are scarce. The standard tools for ROP screening – wide-field retinal cameras like the RetCam – cost upward of $125,0003. They require trained ophthalmologists to operate, and Kenya has around 115 for a population of over 55 million4, more than half of whom are based in Nairobi. Outside the capital, access to specialist eye care is extremely limited. Even where equipment exists, it's shared: hospitals that do have retinal cameras often split one machine between multiple institutions. Indirect ophthalmoscopy, the second standard approach to ROP screening, requires hands-on specialist skill that's even harder to find. For the vast majority of NICUs in Kenya, and in many countries like it, ROP goes unscreened and many premature infants may never receive retinal screening before irreversible vision loss occurs. By enabling nurse-operable bedside imaging, Retinex could help close a critical healthcare access gap and improve long-term outcomes for vulnerable infants in underserved regions.
Designing a portable, nurse-operable retinal screening device for hospitals with limited resources.
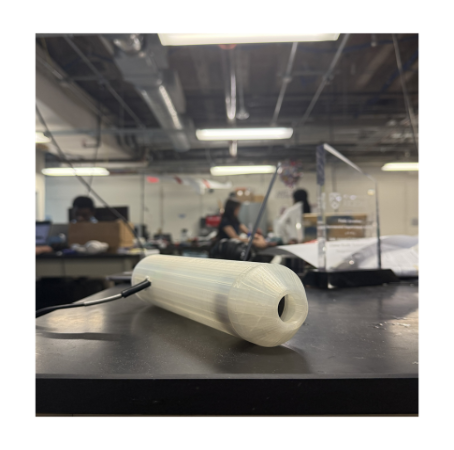
The mission of team Retinex is to design a low-cost, portable, handheld retinal screening device for ROP that works in hospitals with limited resources – one that nurses can operate without specialist training, costs under $500, and is compact enough to be transported and used at the bedside.
The project is developed at Rice University through the EDES 200 engineering design course, and continues work started by a previous student team (IRIS). The current team, consisting of two freshmen and two sophomore students, built the first functional prototype this semester, using off-the-shelf components and keeping the total build cost under $200.

Neonatal retinal imaging presents several difficult engineering constraints simultaneously: small infant pupil size, corneal reflections, thermal safety limits, short working distances, patient motion during imaging, portability requirements, and the need for operation by non-specialists in low-resource settings. The device architecture was designed to balance imaging quality, safety, usability, and low-cost manufacturability within these constraints.
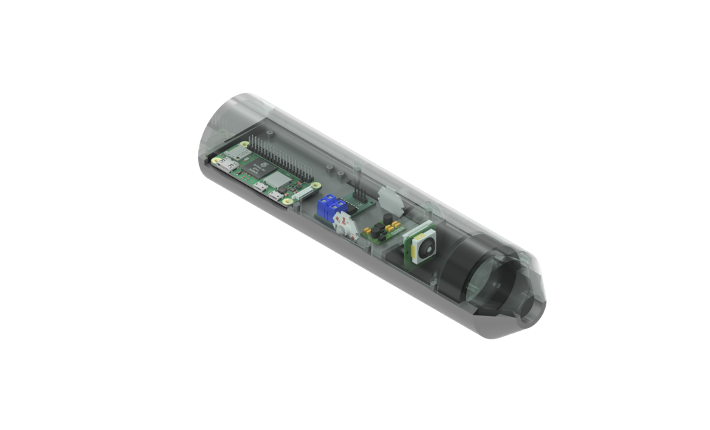
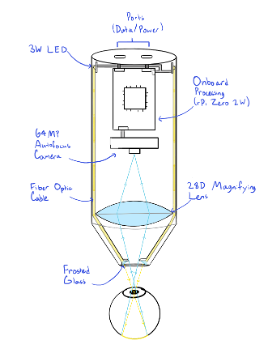
Our solution is a handheld, cylindrical imaging device with four main subsystems: illumination, magnification, capture, and control. The design keeps the form factor compact and the component count low, while addressing the specific constraints of neonatal retinal imaging. This task demands high image quality, safe light exposure, and ease of use in a clinical environment.
Illuminating a premature infant's retina involves a set of competing constraints. You need enough light to image through an infant’s pupil and resolve fine vascular detail at the back of the eye. A heat-generating light source cannot be placed near the infant's face. And specular reflections from the cornea or lens, if not managed, will wash out the very structures you are trying to see.
The device’s illumination system uses a high-output warm LED as the light source. It routes light to the imaging head via a glass fiber-optic light guide, generously donated by Edmund Optics®. The fiber-optic cable physically separates the heat-generating LED from the front of the device, keeping the light-delivery end cool against the infant's face. At the imaging head, the light enters the optical path via a coaxial arrangement aligned with the imaging axis, which largely eliminates corneal and lens reflections that would otherwise degrade image contrast. PWM (Pulse Width Modulation) brightness control is being integrated into the design for precise light-level adjustment; a hands-free foot-pedal interface for use during imaging is currently in development.
The Edmund Optics fiber-optic light guide was a key enabling component for our device. Fiber-optic delivery at this quality and core diameter makes the coaxial design practical at low cost – it provides sufficient optical throughput to illuminate the pupil efficiently while keeping the overall assembly compact. Without it, achieving both safe thermal separation and effective on-axis illumination would require either a significantly more complex optical design or a much larger device.
A 28-diopter ophthalmic lens at the front of the device produces a magnified, real image of the retina. This is the same lens type used in standard indirect ophthalmoscopy, chosen because it provides a field of view greater than 60° within the device's compact geometry. Achieving the full >120° field of view required for comprehensive ROP diagnosis is a key target for future iterations; the current plan is to use image stitching across multiple overlapping captures to reach that coverage.
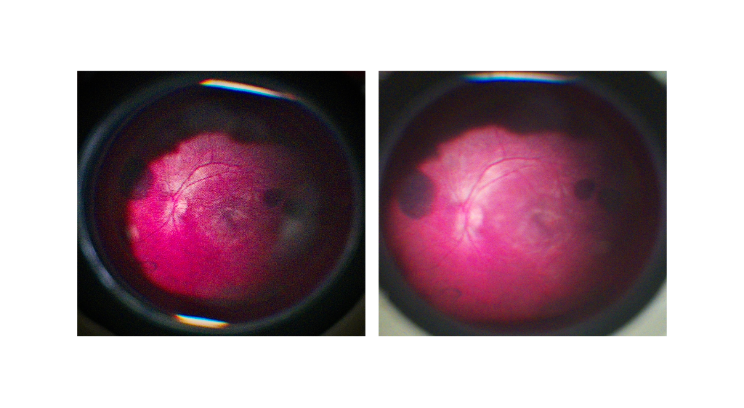
Arducam OwlSight 64MP camera with motorized autofocus and adjustable exposure handles image acquisition. The high pixel count matters in this application because detecting the vascular changes characteristic of early ROP, such as vessel dilation, tortuosity, and ridge formation, requires resolving fine retinal detail that lower-resolution sensors would miss, particularly at the magnification levels involved.
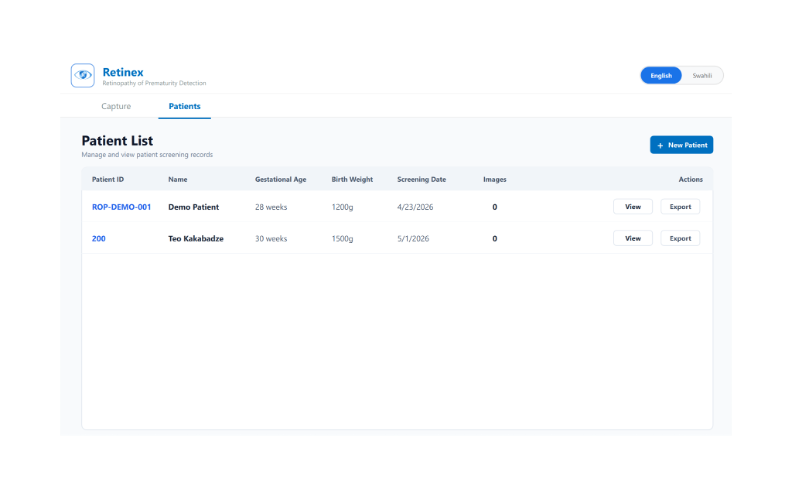
A Raspberry Pi Zero 2W manages all device subsystems: camera exposure and focus, LED brightness, and USB communication with the Retinex Screening App. The app provides a live camera feed for positioning, one-tap image capture, a structured image gallery, and patient data management. Multi-language support is built in, since the device is intended for deployment across different healthcare settings. The interface is designed to be operable by nurses without imaging experience after a short orientation.
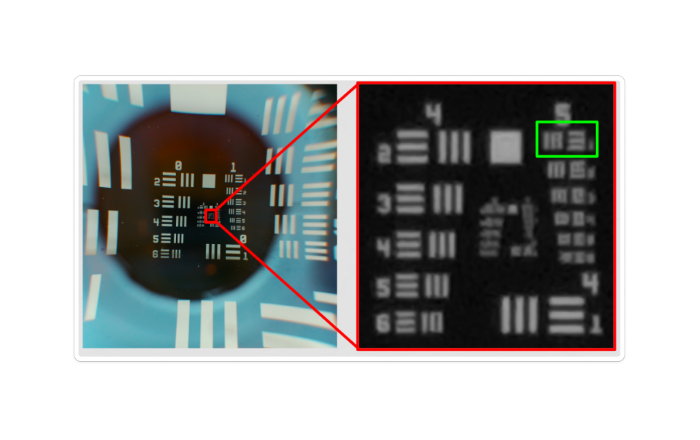
Testing with a USAF 1951 resolution target, the prototype resolves 35.9 line pairs per millimeter. While the ISO 15004-2 standard for ophthalmic imaging instruments specifies a threshold of 60 lp/mm, the achieved resolution is expected to be sufficient to detect the vessel dilation and tortuosity that characterize Plus disease in Zone I. As the innermost retinal region and the site of the most severe ROP presentations, Zone I carries the highest risk of vision loss and represents the most critical target for early diagnosis. The prototype's 60–80° field of view from a single static image is sufficient to cover this region, enabling detection of the most clinically urgent cases of ROP. Full 120° retinal coverage, required for complete disease staging, will be achieved through image stitching in a future iteration. Reaching this clinically relevant diagnostic capability in a first-semester prototype built for under $200 provides a strong foundation for further development and performance improvements.
The project will continue through future Rice University student design teams, with the next phase focused on advancing the system from a functional engineering prototype toward a clinically deployable retinal screening platform.
We thank our sponsor, Harrell Huff, and the Oshman Engineering Design Kitchen at Rice University for their resources and support throughout this project. We are grateful to Edmund Optics for the generous component donation, to Dr. Emmanuel Chang for clinical input on the design, to the EDES 120 team (IRIS) for the work that served as the foundation for this project, and to our faculty mentors Dr. Oden, Dr. Hunter, and Dr. Ghosn.
















or view regional numbers
QUOTE TOOL
enter stock numbers to begin
Copyright 2023, Edmund Optics India Private Limited, #267, Greystone Building, Second Floor, 6th Cross Rd, Binnamangala, Stage 1, Indiranagar, Bengaluru, Karnataka, India 560038
California Consumer Privacy Acts (CCPA): Do Not Sell or Share My Personal Information
California Transparency in Supply Chains Act
This content may include material that has been generated or modified using artificial intelligence (AI).
The FUTURE Depends On Optics®